Brachycephalic Dogs
Most people are not familiar with the term brachycephalic. It describes breeds with short or flat faces such as the Pug, French Bulldog, English Bulldog, Boston Terrier, Pekingese, Shih tzu etc. These breeds are enjoying immense popularity due to their fun, warm natures and eye-catching facial expressions.
Brachycephalic breeds make a lot of snorting respiratory sounds as a matter of course simply because of the way their throats and faces are shaped. These sounds are generated from a combination of several anatomic deformities which have a range of severities.
Research recommends an airway examination under general anaesthesia and possible surgical correction at 4 – 6 months of age. Early intervention prevents ongoing degrees of collapse of the larynx (throat) and reduces the high rates of oesophageal and stomach abnormalities. The aim of all veterinarians is to return the ability to play and exercise like other breeds of dogs without the fear of overheating or collapse especially in the warmer months of the year. This condition does deteriorate with time if untreated thus we have the opportunity to significantly improve their future lives.

Brachycephalic Airway Obstructive Airway Disease (BOAS)
Stenotic Nares
This is a fancy name for narrowed nostrils. The brachycephalic dog’s respiratory passage begins with very small, often slit-like nasal openings for breathing (figure 1). This leads to open-mouth breathing and panting. Affected dogs will especially snore when they are sleeping on their sternums.



Elongated Soft Palate
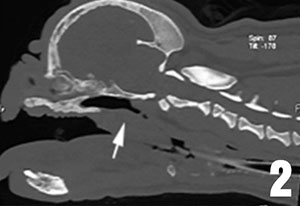
It is difficult to fit the soft palate tissues of the canine mouth and throat into the brachycephalic’s short face. As a result, the soft palate, which separates the nasal passage from the oral cavity, flaps loosely down into the throat. Continual flapping causes inflammation, swelling and thickening thus further restriction to the airway (figure 2 – CT thickened soft palate).


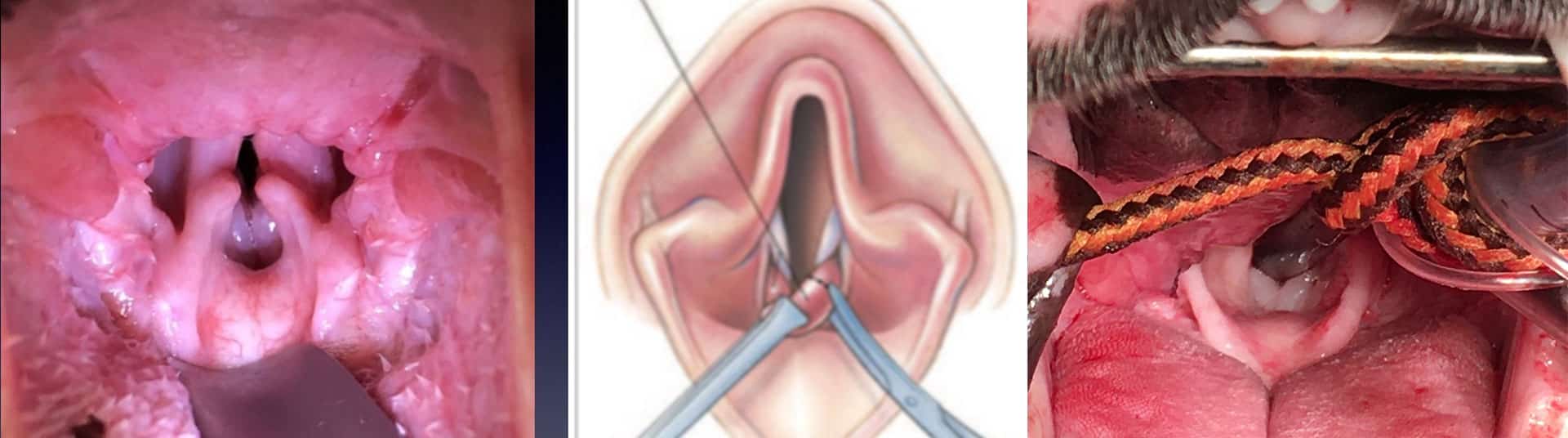
Everted Laryngeal Saccules
The normal larynx has two small pockets called ventricles or saccules. When a dog has increased effort to breathe, over time the linings of these little pockets will turn inside-out within the throat. When this occurs, the protuberances obstruct the throat.
| Study | Stenotic Nares | Elongated Soft Palate | Everted Saccules a | Laryngeal Collapse b |
|---|---|---|---|---|
| Poncet et al 1 | 84.9% (62/73) |
95.9% (70/73) |
54,8% (40/73) |
69.9% (51/73) |
| Poncet et al 2 | 85.2% (52/61) |
100% (61/61) |
54.1% (33/61) |
63.9% (39/61) |
| Torrez and Hunt 3 | 42.5% (31/73) |
86.3% (63/73) |
58.9% (43/73) |
53.1% (34/64) |
| Riecks et al 4 | 56.1% (36/62) |
87.1% (54/62) |
58.1% (36/62) |
8.1% (5/62) |
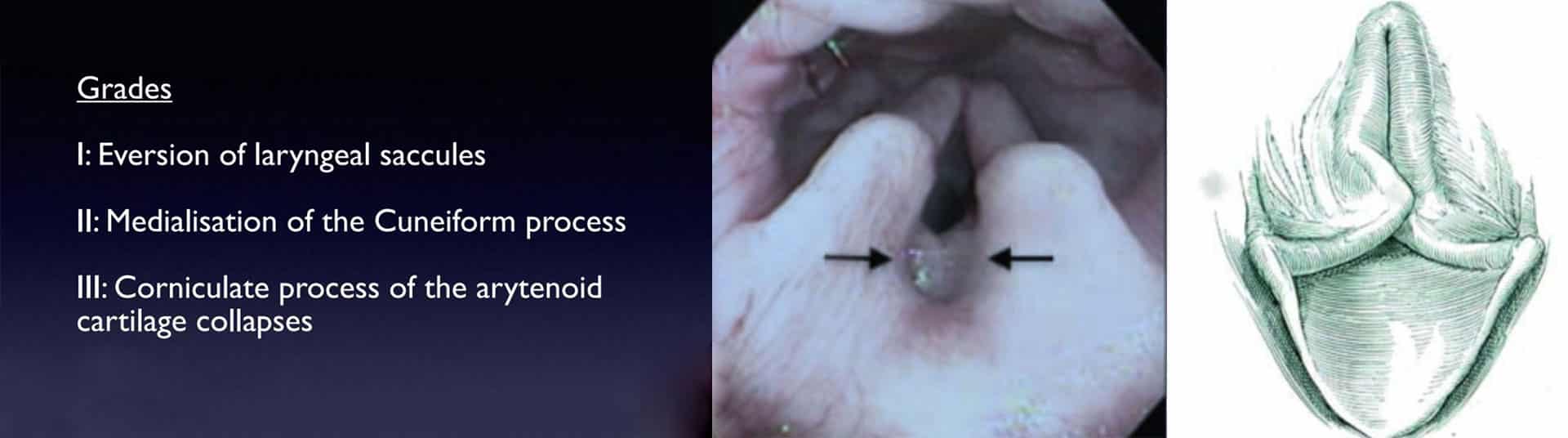
- Stage I Laryngeal Collapse
- Stage II & III Laryngeal Collapse
Gastric and Oesophageal Reflux Diseases
There appears to be a range of stomach and swallowing issues that correlate to the respiratory obstruction suffered by brachycephalic dogs. In these breeds, the oesophagus (the tube that conducts swallowed food from the throat to the stomach) experiences reflux of stomach contents backwards. This reflux generates pain and inflammation. Compounding this problem is retention of food in the stomach for prolonged periods. Medications can be used to manage these issues, should they arise, however surgical correction of the increased respiratory pressures generally leads to great improvement of the gastrointestinal symptoms in approximately 90% of cases. Poiseuille’s law from Physics states that a 50% reduction in tube diameter results in a 16 fold increase in resistance to airflow flow. It is easy to image what the increased sucking pressures to breathe have on the structures of the throat and the oesophageal-stomach junction over time.
Incidence of Stomach and Oesophageal Abnormalities in Brachycephalic Dogs 5 :
- 44% Hiatal Hernia
- 86% Delayed Oesophageal Transit Time
- 75% Gastro-oesophageal Reflux
- 11% Redundant Oesophagus
- 98% Chronic Gastritis (ongoing stomach inflammation
Important Recommendations
- Insure your puppy from 6 weeks of age on first joining the family and check there are no exclusions in the policy for your breed.
- Airway examination at 4-6 months of age; surgical corrections followed by 6 weeks of Losec (Omeprazole – antacid) results in:
- 88% improvement in respiratory signs 2
- 91% improvement in gastrointestinal signs 2
- No fat dogs – obesity further compromises a restricted airway.
- Avoid activity on hot days – brachycephalic dogs pant inefficiently and the extra work required to cool via the tongue can cause the airways to become inflamed and swollen leading to severe obstruction.
- Harnesses are preferable to a lead and collar on walks.
A More Comfortable Life: “Need” Versus “Benefit”
There is a lot of misunderstanding of brachycephalic airways concerns these days. Modern brachycephalic experienced veterinarians now understand the fact that virtually every brachycephalic individual will lead a far more comfortable life, as well as much safer, and potentially longer life with early airway correction before 12 months of age.
WITH THIS IN MIND, MANY PEOPLE WOULD ASK:
“Well why has my dog, and many I know, not needed surgery, and are getting through life ”just fine?”
Let’s consider the fact that all owners of these dogs, most breeders included, accept the following:
- These breeds snore.
- Their sleep is often interrupted through the night. (Is this your dog?).
- Many regurgitate frequently. This can be reduced by smaller feeds, different textures of food and feeding from a height, but in reality, flat faced breeds don’t need to live with this.
- We need to be very careful with these breeds in warm weather.
- These breeds generally don’t exercise as well, or as long, as long-nosed dogs. They may charge around for 15-20 minutes, but then need a rest and are panting in an exaggerated fashion for longer periods than long-nosed dogs.
Society has come to accept all the above as normal, However, all the above happens for one simple reason – almost all these breeds have severe restriction of their airways, resulting in silent suffering. Silent suffering encompasses all the subtle signs listed above that these breeds don’t need to live with, but we expect them to because we accept them as ‘normal’.
Modern experienced veterinarians now realise the benefit of early airway correction. These breeds do not need to live as silent sufferers, as most currently do. With airway correction at under 12 months of age, most of these seemingly normal dogs will not suffer all the above symptoms to nearly the same extent and will lead their most comfortable life. As an owner of one of these breeds, you have a choice to make. Do you accept the above as normal, or do you consider your best opportunity to improve their breathing as much as possible by considering reducing their airway restriction at desexing? Unfortunately, many general practitioners do not understand the above and do not correctly advise owners of their options for the healthiest life at desexing, whereby most owners of these breeds miss their best chance for the healthiest life..
So what do you do?
- If your vet says your brachycephalic pup does not need surgery, or found no problem upon examination at desexing, they unfortunately are highly likely to be wrong, and you could consider a second opinion from a modern experienced brachycephalic veterinarian.
- Before desexing, find and use a surgeon who understands and explains the above to you, and can address all aspects of airway correction.
Extra considerations for Brachycephalic Dogs
Brachycephalic breeds also suffer (to varying degrees), the following conditions that you should at least be familiar with:
- Caudal aberrant turbinates (prolapsed extra folds in the nose)
- Hyperplasic intranasal turbinates (thickened folds in the nose)
- Hypoplastic trachea (narrow windpipe) especially in English Bulldogs
- Hemi-vertebrae (deformed spinal vertebrae)
- Hip dysplasia
The remaining 10% of gastro-oesophageal problems that don’t improve after airway corrective procedures are mostly caused by pyloric stenosis, sliding hiatal hernia or Inflammatory Bowel Disease (food intolerances).